

Background
Phase I study is an essential step of drug development to assess safety, but more recently also to investigate initial insights into potential patient therapeutic response. In the last two decades, treatment of hematologic malignancy has changed dramatically from chemotherapy to targeted agents such as monoclonal antibodies, small molecule inhibitors and immunotherapy. We leveraged a large cohort of phase 1 studies to assess trends in toxicity, response and survival outcomes over time.
Methods
We reviewed the database of all investigator-initiated phase 1 oncology trials treated patients with hematologic malignancies sponsored by CTEP at the NCI between 2000 and 2019. We report the rates of grade 5 toxicity, response to treatment, and survival outcome following enrollment to the trials. Univariate associations of rates of Grade 5 toxicities possibly, probably, or definitely attributable to treatment and response rate with disease type, year of study activation, or whether each type of treatment was administered were assessed through likelihood ratio tests of a generalized linear mixed model.
Results
Overall, 3,308 patients were treated in 161 trials. Median age of the patients was 61 (range: 0-96) and 61% were male. Acute myeloid leukemia/myelodysplastic syndrome (AML/MDS) was the most common enrolled malignancy diagnosis (N=1,768) followed by lymphoma (N=921), acute lymphoblastic lymphoma (ALL: N=193) and myeloma (N=153). Forty percent of the trials used an investigational agent as a monotherapy, while 60% of the trials used combination treatment. The most commonly used non-chemotherapy investigational agents were monoclonal antibodies and HDAC inhibitors (28 trials each), followed by DNMT inhibitors (18 trials) and proteasome inhibitors (17 trials).
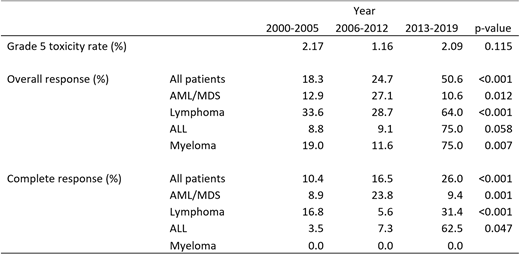
Overall, 468 patients died during trials of which 60 were attributed to the treatment (grade 5 toxicity: 1.81%, 95%CI: 1.36-2.27%). There was a trend of higher grade 5 toxicity in patients with AML/MDS (2.43%) compared to patients with lymphoma (0.98%), ALL (1.55%) or myeloma (0.65%) (p=0.066). Treatment with a PD-1 inhibitor was associated with significantly higher risk of grade 5 toxicities (7.14%, 95%CI: 1.95%-12.3%), compared to patients who did not receive a PD-1 inhibitor (1.65%, 95%CI: 1.21%-2.09%) (odds ratio [OR]: 4.93, 95%CI: 1.54-15.8). The deaths mostly occurred in trials combining a PD-1 inhibitor and a CTLA-4 inhibitor (6 death in 77 pts), although the grade 5 toxicity rate did not significantly differ from PD-1 inhibitor monotherapy (1 death in 21 pts). There was no significant difference in grade 5 toxicity among the time periods when trials were activated (Table. 2000-2005 vs 2006-2012 vs 2013-2019). Baseline characteristics associated with higher risk of grade 5 toxicity were age (OR: 1.02 by 1 year increase in age, 95%CI: 1.01-1.04, p=0.007) and performance status ≥2 at enrollment (OR: 1.56, 95%CI: 1.02-2.39, p=0.039).
Response assessment was available in 2,404 patients. Overall response rate (ORR) and CR rate (CRR) from all trials were 25.1% (95%CI: 23.3-26.8%) and 14.7% (95%CI: 13.3-16.2%), respectively. The patients with lymphoma experienced significantly higher ORR (42.8%) compared to patients with AML (18.2%), ALL (13.3%) or myeloma (13.3%). There is a significant increase in both ORR and CRR over time (Table. p<0.001), but the trend of change was different in each disease by investigational agents tested during the period. Monoclonal antibodies, iMIDs, CDK inhibitors and BTK inhibitors were non-chemotherapy agents associated with higher response rate.
Overall survival (OS) was available in 2,664 patients. The median OS among all patients after enrollment in phase 1 studies was 277 days (95%CI: 245-305 days). Patients with ALL had significantly shorter median OS (86 days) compared to patients with AML/MDS (255 days), lymphoma (289 days) or myeloma (median not reached).
Conclusion
There has been a significant improvement of ORR in CTEP sponsored phase I studies in the last 20 years. Grade 5 toxicity rate remained low, but higher age and poor performance status were associated with higher risk. Participation in phase I studies should be encouraged in patients with hematologic malignancies.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal